Printable Cna Shower Sheets Form in PDF
Printable Cna Shower Sheets Form in PDF
Form 4562 Example - The form is often required to apply for business loans or grants, as it shows the business’s financial performance.
To facilitate the sale of a vehicle in Wisconsin, it is essential for both the seller and the buyer to complete the Motor Vehicle Bill of Sale form. This document ensures a clear record of the transaction, safeguarding both parties in terms of ownership and legal accountability. For those looking to streamline this process, you can download the form now and ensure all necessary details are accurately captured.
Ca Dmv Reg 256 - Contact information is collected to facilitate communication regarding the application status.
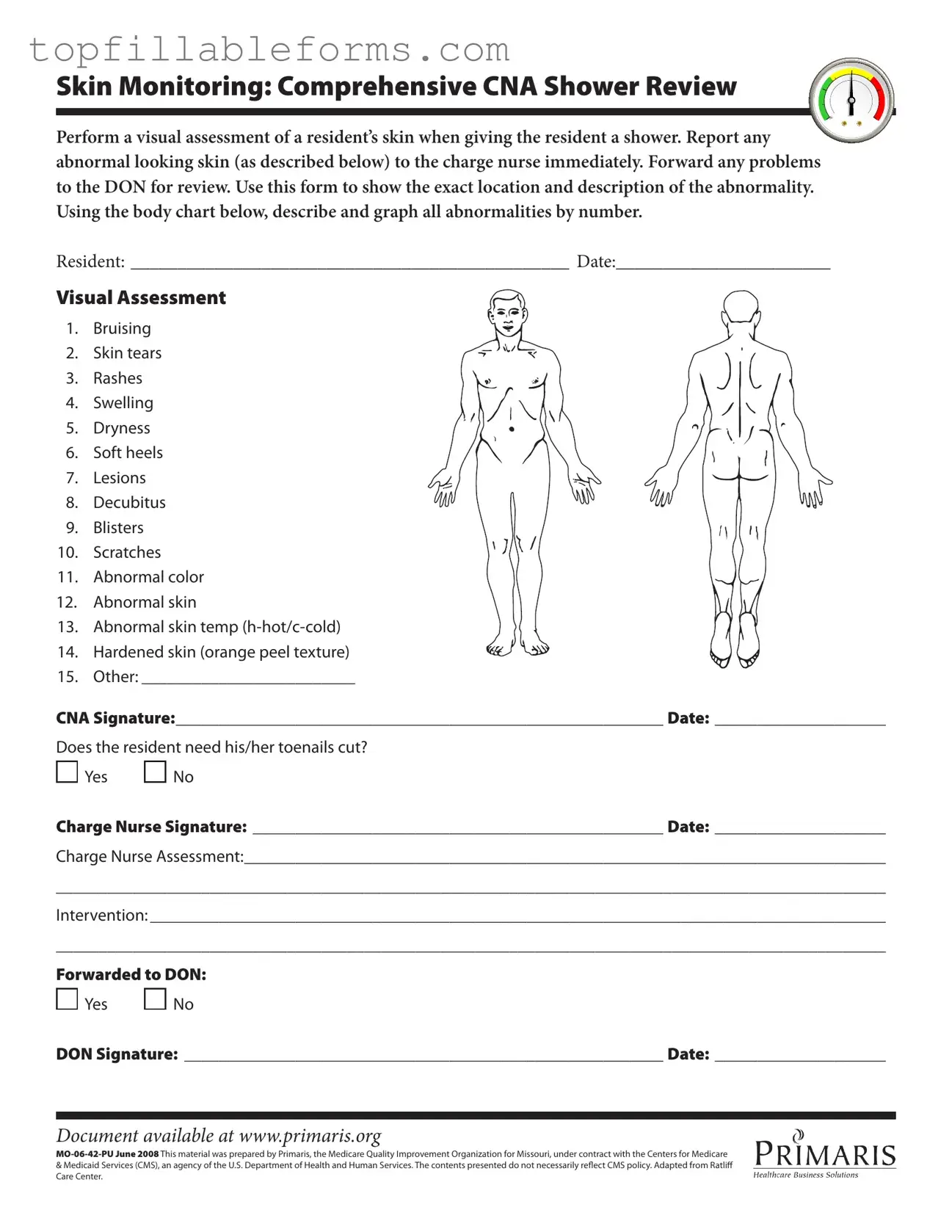
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
In the realm of healthcare documentation, particularly in facilities like nursing homes, various forms work together to ensure comprehensive care and accurate reporting. The CNA Shower Sheets form is crucial for monitoring residents' skin health during showers. However, it often accompanies several other documents that enhance the overall care process. Below are some commonly used forms that complement the CNA Shower Sheets.
Together, these forms create a robust framework for monitoring and documenting residents' health, particularly regarding skin integrity. By utilizing these documents, healthcare providers can ensure that they deliver thorough and attentive care, ultimately enhancing the quality of life for residents.
Misconceptions about the CNA Shower Sheets form can lead to confusion and improper use. Here are four common misunderstandings:
Many believe that the CNA Shower Sheets form is only necessary for serious conditions like deep wounds or infections. In reality, it is essential for recording all skin abnormalities, including minor issues like dryness or minor bruising. Every detail matters, as early detection can prevent more significant problems.
Some think that only the charge nurse has the authority to fill out the form. However, CNAs play a critical role in the initial assessment. They are responsible for documenting their observations and reporting them to the charge nurse, who then adds their assessment and any necessary interventions.
This is a dangerous belief. The CNA Shower Sheets form is a required part of the care process. Even if a resident appears to have healthy skin, a visual assessment must still be conducted. Regular documentation helps maintain a comprehensive record of the resident's skin health over time.
Some individuals may think the body chart is merely illustrative. In fact, it is a crucial component of the form. Accurately marking the location and type of skin abnormalities helps ensure that all team members are aware of specific issues and can monitor changes effectively.
The CNA Shower Sheets form is designed to facilitate a thorough visual assessment of a resident's skin during their shower. This form serves as a tool for Certified Nursing Assistants (CNAs) to document any abnormalities they observe, such as bruising, rashes, or lesions. By recording these details, the form helps ensure that any potential issues are promptly reported to the charge nurse and addressed accordingly.
The body chart is an essential component of the CNA Shower Sheets form. CNAs should use it to mark the exact locations of any abnormalities they identify on the resident's skin. Each abnormality should be numbered and described clearly. This visual representation aids in communication with the charge nurse and helps track changes over time.
CNAs should be vigilant in observing various types of skin abnormalities during the shower. The form lists several conditions that require attention, including bruising, skin tears, rashes, swelling, and dryness, among others. Any abnormal color, temperature, or texture of the skin should also be documented. Reporting these issues promptly can prevent further complications and ensure the resident receives appropriate care.
If a CNA observes any abnormalities during the skin assessment, they must report these findings to the charge nurse immediately. This is crucial for ensuring the resident's health and safety. After the charge nurse reviews the situation, any necessary interventions should be documented on the form. Additionally, the information may be forwarded to the Director of Nursing (DON) for further evaluation.
Yes, the CNA Shower Sheets form includes a specific question regarding whether the resident needs their toenails cut. This section allows CNAs to ensure that all aspects of the resident's personal care are addressed. If the answer is yes, it can prompt further action to ensure the resident's comfort and hygiene.
The form requires several signatures to ensure accountability. The CNA must sign and date the form after completing the assessment. The charge nurse also needs to sign and date it after reviewing the findings. If the situation is escalated to the DON, their signature is required as well. This multi-signature process helps maintain a clear chain of communication and responsibility in resident care.