Printable Medication Administration Record Sheet Form in PDF
Printable Medication Administration Record Sheet Form in PDF
Broward County Animal Care and Adoption - Being prepared with this certificate can lead to a smoother pet ownership experience.
Where Can I Get a Trust Amendment Form - This form can help clarify roles and responsibilities associated with the trust.
For individuals looking to manage liability effectively, it is vital to understand the implications of the Hold Harmless Agreement and how it can serve as a protective measure in various activities. Many seek to utilize this form to ensure clear responsibilities and protections in their engagements. Explore further details in the context of this important legal document through the key Hold Harmless Agreement insights.
Dekalb County Water New Service - Use this application for changes in water service billing preferences.
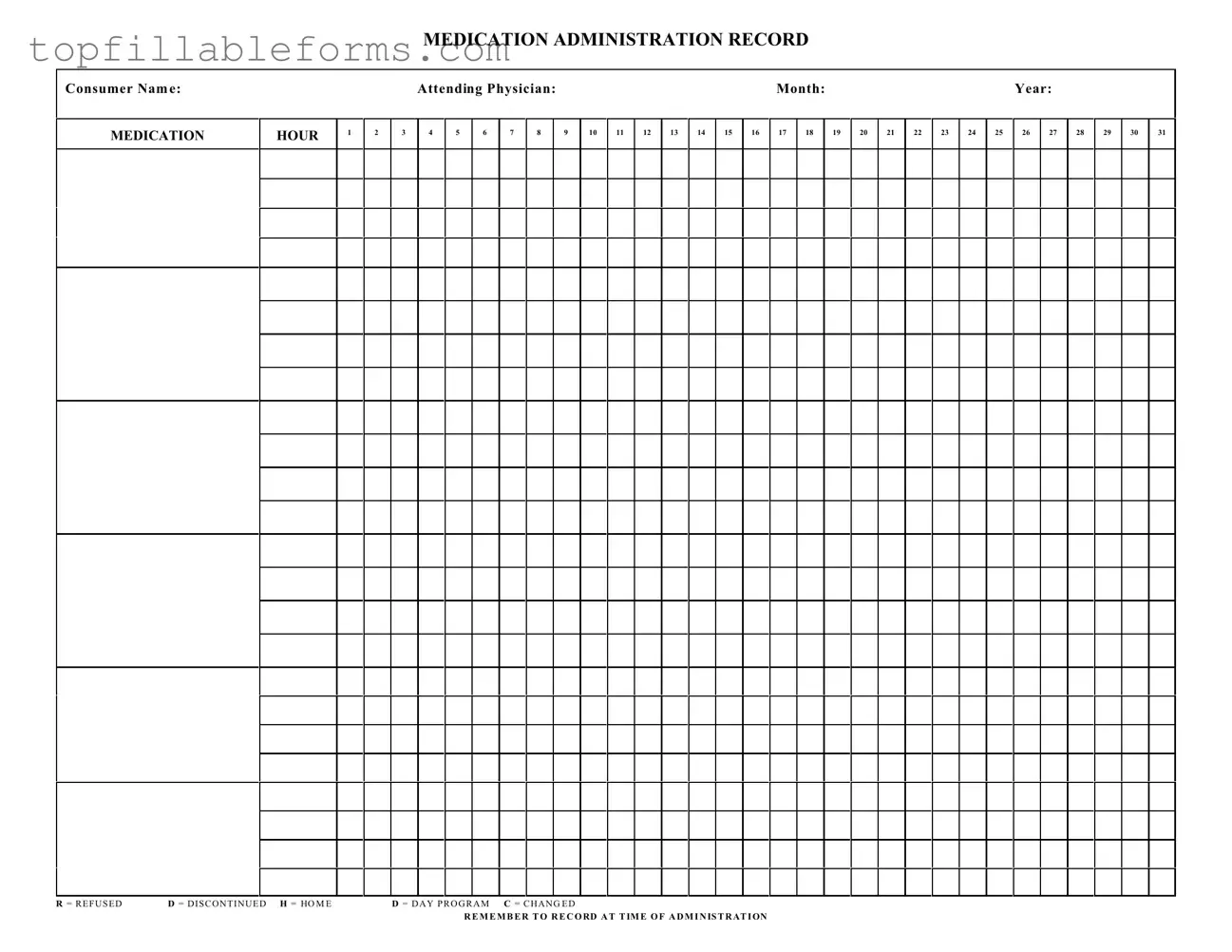
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
The Medication Administration Record Sheet is a crucial document in managing patient medications. However, several other forms and documents are often used in conjunction with it to ensure comprehensive care and accurate record-keeping. Below are five important documents that complement the Medication Administration Record Sheet.
These documents work together to create a complete picture of a patient's medication management. Proper use of each form enhances communication among healthcare providers and ensures patient safety.
The Medication Administration Record Sheet is an essential document used in healthcare settings to track medication administration. Several other documents serve similar purposes, ensuring proper medication management and patient safety. Here are seven documents that share similarities with the Medication Administration Record Sheet:
Understanding the Medication Administration Record Sheet form is essential for proper medication management. However, several misconceptions can lead to confusion. Below are nine common misconceptions and clarifications regarding the form.
Being aware of these misconceptions can help ensure proper use of the Medication Administration Record Sheet form, ultimately contributing to better patient care.
The Medication Administration Record Sheet (MARS) is a vital tool used to track the administration of medications to individuals. It ensures that medications are given at the correct times and allows caregivers to document any changes in the medication regimen.
This form is primarily used by healthcare providers, caregivers, and family members responsible for administering medications. It is especially useful in settings like nursing homes, assisted living facilities, and home care environments.
Begin by entering the consumer's name, the attending physician's name, and the month and year. Then, for each medication, record the time it was administered in the designated hour columns. If a dose is refused, discontinued, or changed, use the provided codes (R, D, H, C) to indicate the status of each medication.
Documenting the time of administration is crucial for ensuring that medications are taken as prescribed. It helps prevent potential overdoses or missed doses, which can have serious health implications. Accurate records also facilitate communication among healthcare providers.
If a medication is refused, mark the appropriate code (R) in the record sheet. It is also essential to note the reason for refusal, if known, and to inform the attending physician or healthcare provider to discuss any necessary adjustments to the treatment plan.
While the MARS is designed for individual use, you can create separate sheets for each consumer. This approach ensures that each person's medication history is accurately documented and easily accessible, which is essential for effective care.
Completed sheets should be stored securely in a confidential manner to protect the privacy of the individual. They should be easily accessible to authorized personnel who may need to review the medication history for ongoing care.
If an error occurs, do not erase or use correction fluid. Instead, draw a single line through the mistake and write the correct information next to it. Initial and date the correction to maintain an accurate record. This practice ensures transparency and accountability in medication administration.